UNIT 19
15 Vision
Vision is the perception of light through the eye-brain system-a rather dry definition for the most amazing and complex of our senses. Three major disciplines are involved in any complete description of vision. Physics describes light and how an image is formed on the retina. Physiology describes how the image is processed by the eye-brain system. Perceptual psychology deals with higher-level processing of the information and subsequent formation of a perception. This chapter concentrates on the physics of image formation and vision correction, including some elementary physiology of the eye. The last section of this chapter, on color vision, introduces the subject of color and gives an indication of how complex the sense of vision is.
15.1 IMAGE FORMATION BY THE EYE
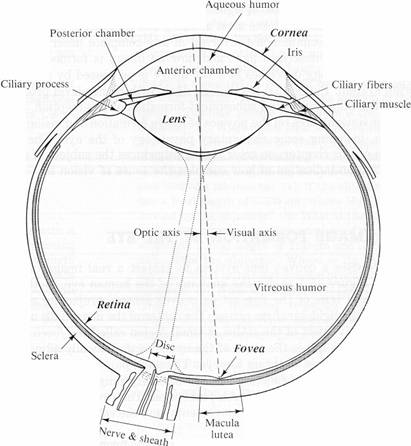
The eye uses a convex lens system to project a real image on the retina. Figure 15.1 shows the anatomy of the human eye. Both the cornea and lens of the eye act as convex lenses, projecting a real image on the light-sensitive retina. The center of the image falls on the most sensitive part of the retina, a small region called the fovea. The opening in the iris is the pupil of the eye. It automatically adjusts to the amount of light entering the eye. The pupil plus chemical adaptation allow the eye to function over an intensity range of 1010:1. The two eyes together provide depth perception. The eyes also sense the direction in which they point, movements, and the color of objects and light sources.
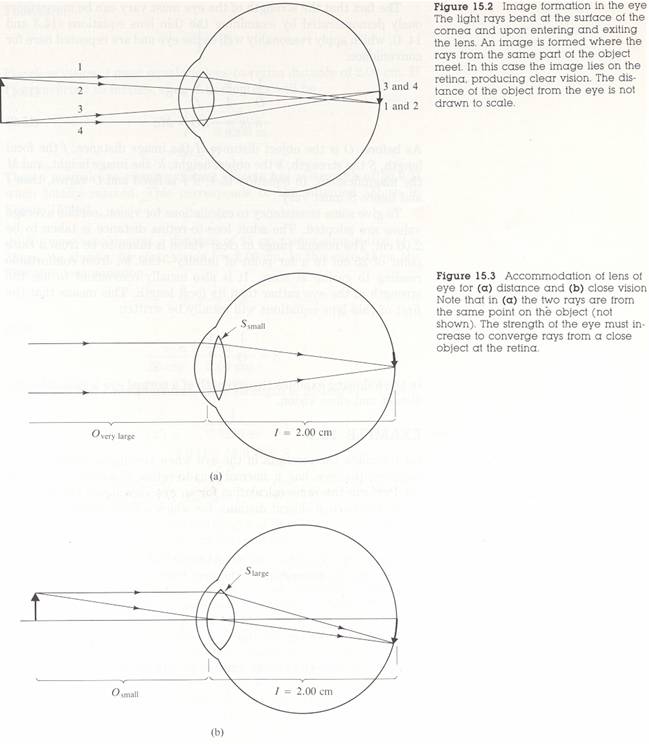
The ray diagram in Figure 15.2 shows image formation by the cornea and lens. The cornea does roughly two-thirds of the bending of rays. The lens does the remaining fine tuning necessary to produce an image on the retina. Light rays pass through many layers of materials (air, cornea, aqueous humor, lens periphery, lens core, lens periphery, and vitreous humor) on their way to the retina, changing direction at each interface. However, the indices of refraction of the materials involved are such that significant bending occurs only at the cornea and lens. Furthermore, the cornea and lens can be treated as a single lens with- a strength equal to the sum of their individual strengths, a tremendous simplification.
Accommodation
For an object to be seen clearly, its image must lie precisely on the retina. In slightly more quantitative terms this means that the image distance I must equal the lens-to-retina distance for clear vision. Because the lens-to-retina distance in the eye does not change, the image distance I must be the same for all objects at all distances. The only way the eye can do this is to vary its focal length, and hence its strength, to accommodate various object distances. The process is thus called accommodation.
|
|
Figure
15.1
Cross-sectional anatomy of the human eye seen from above. (Adapted from
Theodore D. Ruche and Harry C. Patton, Physiology and Biophysics, 19th ed.
Saunders, Philadelphia,1965, by permission.)
Figure 15.3 illustrates how the strength of the eye varies for distant and close objects. Rays of light from a distant object, as shown in Figure 15.3(a), are nearly parallel, and the eye is easily able to converge them on the retina. Rays from a close object can diverge and still enter the eye, as seen in Figure 15.3(b). The eye must therefore be more converging to cause the rays to meet on the retina when viewing a close object. A more-converging lens has greater strength, as indicated by the thicker lens for close vision. Muscle action in the eye adjusts the thickness and strength of the lens, doing the fine tuning necessary to produce an image precisely on the retina. The muscle is relaxed for a thin lens and tensed for a thick lens. Distant vision is thus termed totally relaxed and close vision is termed accommodated.
The fact that the strength of the eye must vary can be more rigorously demonstrated by examining the thin lens equations (14.3 and 14.4), which apply reasonably well to the eye and are repeated here for convenience:
![]() (15.1)
(15.1)
![]() (15.2)
(15.2)
As before, O is the object distance, I the image distance, f the focal length, S the strength, h the object height, h' the image height, and m the magnification. In equation 15.1, if I is fixed and O varies, then f and hence S must vary.
To give some consistency to calculations for vision, certain average values are adopted. The adult lens-to-retina distance is taken to be 2.00 cm. The normal range of clear vision is taken to be from a close point of 25 cm to a far point of infinity-that is, from comfortable reading to gazing at stars. It is also usually convenient to use the strength of the eye rather than its focal length. This means that the first of thin lens equations will usually be written
![]() .
.
Acuity
Visual acuity is the sharpness of detail detectable with the eye - a property physicists call optical resolution. Vision tests, such as reading lines of letters on a chart, assume a certain acuity is normal. A patient's eyes are tested against this norm to ascertain whether vision correction is called for. How fine a detail can the normal eye discern? And what prevents the eye from resolving even smaller detail? The answers to these questions give some insight into how sophisticated an instrument the eye is.
The various methods of measuring visual acuity yield somewhat different results. They are all roughly consistent, however, and correspond to the ability to resolve detail as small as the diameter of a human hair held at arm's length. This is impressive in itself, but it is even more impressive when the size of images on the retina are considered.
15.2 CORRECTION OF COMMON VISION DEFECTS
A majority of people need some kind of vision correction. The most common vision defects are simple in nature and easily corrected with spectacle lenses. Vision correction has been performed for many centuries. Spectacle lenses are known to have been used as early as the fourteenth century, and cataract removal was practiced by the Romans and possibly in earlier civilizations. Only in the last hundred years or so has vision correction become available to other than the very rich.
The most common vision defects are myopia (nearsightedness) and hyperopia (farsightedness). Figure 15.6 illustrates these defects. The cause of both defects can be either a lens of incorrect strength or an eye of incorrect length. Small imperfections, such as an eye that is 0.01 cm too long or a lens that is 0.5 D too strong, cause noticeable vision deficiencies.


Myopia
A myopic person can see close objects clearly, but distant vision is blurry-hence the common term nearsightedness. As shown in Figure 15.6(a), parallel rays from a distant object converge before they meet the retina and are diverging again at the retina. The myopic eye cannot relax its lens enough to avoid overconverging rays from a distant object. If the eye is a normal (length lens-to-retina distance of 2.00 cm), this means that the strength of the fully relaxed eye is greater than 50.0 D. To correct for myopia, a spectacle lens of negative strength is used, as shown in Figure 15.7(a).

Figure
15.7 (a) Correction for myopia: A diverging lens is used since the eye is too
converging. (b) Correction for hyperopia: A converging lens is used since the
eye is not converging enough. The heavy lines are the paths that the rays take
with a spectacle lens in place; the thinner lines are the paths without a
spectacle lens.
Hyperopia
A hyperopic person can see distant objects clearly, but close objects are blurry-hence the common term farsightedness. As shown in Figure 15.6(b), rays from a close object do not converge by the time they strike the retina. The lens of the hyperopic eye has insufficient strength to converge rays from a close object on the retina, even when fully accommodated. For an eye of normal length this means that the maximum strength of the eye is less than the needed 54.0 D. To correct for hyperopia, a spectacle lens of positive strength is used, as shown in Figure 15.7(b).
Loss of Accommodation Ability: Presbyopia
The ability to accommodate decreases with age. The onset of presbyopia, which literally means "old eye," usually is noticed when reading materials must be held at arm's length to be legible. Distant vision usually is not affected, just the ability of the lens of the eye to increase its strength. The loss of accommodation ability is attributed primarily to stiffening of the lens. Presbyopia eventually affects nearly everyone, whether their eyes are normal, myopic, or hyperopic.
One correction for presbyopia is the use of bifocals. A bifocal lens is ground to two different curvatures. The bottom part of the lens has a greater strength than the top since we generally look downward at close objects and need greater strength to see them. Bifocals reputedly were invented by Benjamin Franklin. Trifocals are also used, but they are harder to adapt to. Other possibilities are different glasses for viewing different distances or half-lens reading glasses (which are also useful for peering over and looking thoughtful).
Astigmatism
In astigmatism, another very common vision defect, the cornea or lens of the eye is not symmetric. Figure 15.8 shows a chart used to detect astigmatism. To a person with astigmatism, some lines appear darker and sharper because they are properly focused while other lines are not. Figure 15.9 shows how an astigmatic lens affects rays from a distant object.

Figure
15.8 Chart for detecting astigmatism. If some of the lines appear darker or
clearer to you than others when viewed without corrective lenses, you have an
astigmatism. Check each eye separately and look at the center cross.
Astigmatism often can be corrected by using a spectacle lens with the opposite asymmetry of the astigmatic eye. For example, if the astigmatic lens is too strong vertically and too weak horizontally (Fig-15.9), a lens that is diverging vertically and converging horizontally will correct the problem. Astigmatism corrections are accomplished by adding a cylindrical lens to the normal lens of the spectacle. Cylindrical lenses look as if they were cut from a can (cylinder) rather than from a sphere. An eyeglass prescription for astigmatism specifies the cylinder strength in diopters and its orientation (determined using the chart in Figure 15.8). Corrections for myopia or hyperopia are made in the same lens that corrects astigmatism. Corrections for myopia and hyperopia are specified as spherical (symmetric) corrections, also in diopters. Contact lenses ordinarily have no correction for astigmatism because of the difficulty in orienting the lens. Contact lenses can be used to reshape the cornea, and surgery may also be performed on the cornea to correct astigmatism, myopia, or hyperopia.

Figure
15.9 The astigmatic lens: Rays striking the vertical line on the lens cross
close to the lens. Rays striking the horizontal line on the lens cross much
further from the lens. All rays come from the same point on a distant object.
This lens can be considered too strong along its vertical axis and too weak
along its horizontal axis.
Cataracts
A cataract is an opacity of the lens of the eye. Cataracts are common in the elderly, but their advent can be hastened by exposure to ultraviolet radiation, microwaves, nuclear radiation, and certain chemicals. The cloudy lens must be removed, as it is not possible to make it clearer again. Once the lens is removed, the patient needs glasses with a large positive strength. In addition, the eye then totally lacks accommodation ability and bifocals are routinely prescribed. If only one is affected, then binocular (two-eye) vision becomes difficult because the strong positive lens magnifies everything seen by the affected eye. In recent years artificial lenses have been implanted in place of the removed lens with great success. The patient still requires bifocals, but vision is more easily corrected and objects in the field of view are not as magnified as they are with an external lens.
Other recently developed methods of vision correction include the use of lasers to spot-weld detached retinas. The lens of the eye is used to focus the laser beam on the desired spot, and the scar tissue from small burns forms "welds." Electrical devices are even being used to stimulate the optic nerve artificially. This can give a very primitive
sense of vision, but it may be improved in the future.
There are many other less-common vision defects not easily corrected by simple spectacle lenses. The references at the end of chapter explore the subject of vision correction in greater depth.